Indole Analys
Disorders of Tryptophan
Disorders of Tryptophan intestinal resorption, transport and metabolism can cause severe Somatic, Neurological and Behavioural Abnormalities.
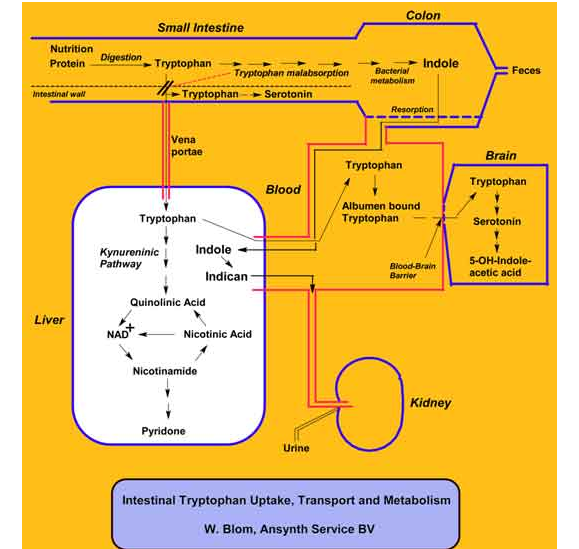
- Intestinal malabsorption of tryptophan can lead to tryptophan deficiency. An excess of tryptophan is then entering the colon, and is metabolized or gradated by colonic bacteria. One important degradation reaction is the conversion of tryptophan into free indole by splitting of the alanine side-chain. Indole absorbed by the colon, will be transported by the great blood circulation to the liver. In the liver indole is sulfonated to indican (= 3-indolesulfonic acid). Indican is excreted in the urine by the kidney. A high excretion of indican in the urine, mostly combined with a low urinary tryptophan, is a symptom of tryptophan malabsorption in the small intestine. See Figure 1.
{kind=link}
- Intestinal tryptophan malabsorption leads to defecation problems, because the serotonin synthesis in the intestinal wall is decreased, which causes less peristaltic movement.
- Tryptophan deficiency in the liver decreases the production of NAD+ via the kynurenine pathway. The result will be a lower level of NAD+ catalysed oxidation processes and diminished production of ATP. This has e.g. as consequence that intracellular enzyme ATP-ase with cofactors ATP and Mg2+ needed for the Na+/K+-pump and Ca2+/Mg2+-pump is not working properly. These Ion-pumps are very important for the regulation of the osmolarity within the cell and the working of Ion-channels in relation to neurotransmission. A low production level of NAD+ and ATP are responsible for a lot of clinical problems. By measurement of tryptophan, kynurenine pathway metabolites, indican and other indole metabolites in urine, the metabolic consequences of tryptophan deficiency can be indicated.
- Tryptophan deficiency in blood results also in a lower level of tryptophan transport over the blood/brain barrier. This will decrease the tryptophan availability as precursor for the serotonin biosynthesis in the central nervous system, leading to serotonin neurotransmission problems. The tryptophan analysis of free and bounded tryptophan in blood might indicate a lower tryptophan transport over the blood/brain barrier.
By measurement of amino acids and free + total tryptophan in blood, and amino acids + tryptophan and many metabolites in urine a specialist can indicate the severity of nutritional deficiencies, and tryptophan transport and metabolism disorders.
Somatic
- Anorexia
- Glossitis
- Constipation or diarrhea
- Dermatitis
- Pellagra-like skin problems
Neurological
- Neurological
- Epilepsy
- Bulbar palsy
- Tremor
- Loss of position sense
- Spasticity
- Exaggerated tendon reflexes
- Hyperesthesia
- Paresthesia
Behavioural
- Apathy
- Anxiety
- Depression
- Obsession- compulsion
- Hostility
- Hyperirritability
- Mania
- Memory deficits
- Delirium
- Organic dementia
- Emotional lability
- Sleep difficulties
- AD or ADHD
- Autism like symptoms
Note: Depending on age, nutritional status or severity of deficiencies, and/or metabolic abnormalities not every symptom needs to be present, or the symptoms differentiates in severity.